- 000 - 123 - 456789
- info@trustaclinic.ae
- VILA 17, Street 73B, AL SATWA, Dubai, UAE

CONTACT US
- (000) 123-456-789
- VILA 17, Street 73B, AL SATWA, Dubai, UAE.
- info@trustaclinic.ae
Shoulder Arthroscopy in Dubai
There is a particular kind of frustration that comes with a shoulder problem that just will not resolve. It is not always dramatic. Sometimes it is a dull ache that shows up whenever you try to sleep on that side. Sometimes it is weakness that catches you off guard mid-movement. Sometimes it is a clicking, catching sensation that has become so familiar you have stopped mentioning it to people. You just work around it.
The patients we see in Trusta Clinic Dubai have usually been working around it for a while. They have rested, stretched, done their physiotherapy sessions, maybe had an injection. Some improved for a few months and then regressed. Others never really got ahead of it. By the time they come in to see us, they are not looking for another short-term fix. They want to know if there is a proper, lasting solution.
For many of them, shoulder arthroscopy is exactly that.
The Procedure Itself
We could start with the technical definition, but honestly the more useful thing is to explain what it feels like from the patient side.
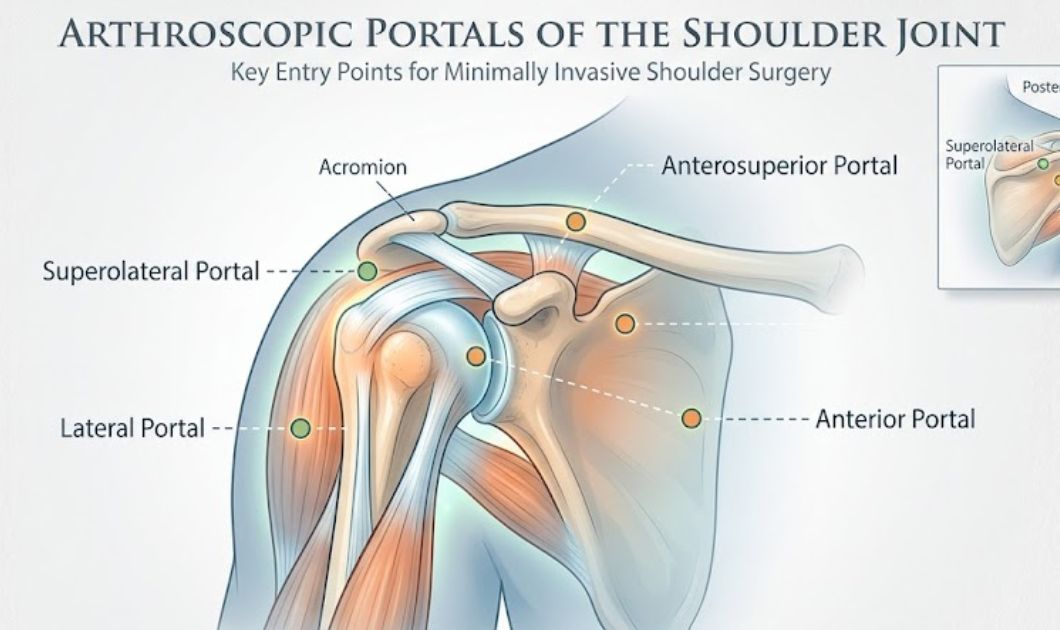
You come in on the day of surgery. Anaesthesia is administered. Two to four small openings, each about a centimetre wide, are made around the shoulder. Through one of them, our surgeon passes a thin instrument called an arthroscope, which carries a camera at its tip and sends live images to a screen in the operating room. The other openings allow miniature tools to be passed in to carry out whatever repair is needed.
The entire interior of the joint becomes visible in real time. Every tendon, every patch of cartilage, the joint lining, the ligaments. Our surgeon examines all of it before touching anything. Then the repair work begins, guided throughout by what is on that screen rather than by feel through a large incision.
When it is done, the small openings are closed, a dressing goes on, the arm goes into a sling. Most patients go home the same day, sometimes a few hours after waking from anaesthesia.
The difference between this and traditional open shoulder surgery is substantial. Open surgery requires cutting through the overlying muscle and soft tissue to access the joint. That tissue has to heal on top of whatever the actual problem was, which makes recovery longer, more painful, and more complicated. Shoulder arthroscopy sidesteps most of that. The joint gets fixed. The body has much less additional damage to deal with while it heals.
What We See and Treat Inside the Joint
People sometimes assume shoulder arthroscopy is for one specific condition. It is actually used for quite a range of problems, and often more than one issue is found and addressed in the same session.
Rotator cuff tears are among the most common things we deal with. The rotator cuff is a group of four tendons that stabilise the joint and power most arm movements. When one of these tears, whether from a single traumatic event or from years of accumulated strain, the shoulder loses strength in ways that are hard to compensate for. Reaching behind your back, lifting overhead, throwing, pressing, all of these movements become unreliable or painful. Arthroscopic tendon repair surgery reattaches the torn tendon to the bone using small anchors. The recovery is real and takes commitment, but the restoration of function at the end of it is significant. Patients regularly tell us they had stopped expecting to use the shoulder normally again.
Shoulder impingement comes up constantly. The tendons of the rotator cuff pass through a narrow channel beneath a bony arch at the top of the joint. When that space tightens, the tendons get repeatedly pinched during movement. The characteristic catching pain when lifting the arm is something many patients have been managing for months or years by the time they reach us. During arthroscopy we decompress the space by removing whatever is causing the compression, whether that is a bone spur, thickened tissue, or both. The relief after this one tends to come early and clearly, which patients find enormously satisfying after a long stretch of grinding discomfort.
Labral tears, including SLAP injuries, are something we see a lot in active patients. The labrum is a rim of cartilage around the shoulder socket that gives the joint its depth and stability. When it tears, things feel off in a way that is difficult to describe precisely. Loose. Unreliable. Sometimes there is a catching sensation. SLAP tears in particular affect the top of the labrum and are especially common in people who throw, swim, or play racket sports. Arthroscopic repair here gives us a level of precision that simply would not be achievable through an open incision.
Recurrent dislocations are a different category of problem but one we treat regularly. After a shoulder dislocates once, the structures holding it in place are often stretched enough that the threshold for it happening again drops significantly. Some patients arrive having had the shoulder pop out four or five times, sometimes from movements as minor as reaching for something. Arthroscopic stabilisation surgery tightens and reattaches what should be holding the joint in position. For most patients it ends the cycle that has been making them guard the shoulder constantly.
Frozen shoulder deserves its own mention because the experience of it is so consistently miserable. The joint capsule becomes inflamed and thickened, and the shoulder locks up. Getting dressed, reaching a shelf, rolling over in bed. All of it hurts. Sleep becomes fractured and exhausting. When physiotherapy and injections have been given a genuine trial and have not freed things up, an arthroscopic capsule release can change the picture rapidly. The range of motion that returns in the first few weeks after this procedure genuinely surprises some patients. They had adjusted their expectations downward over months of slow progress, and the speed of improvement catches them off guard.
We also deal regularly with bursitis and bone spurs, both of which produce that persistent background irritation that rest never fully resolves, and with AC joint problems from contact sport, falls, or long-term overhead strain.
Is This the Right Step for You
The honest answer is that it depends, and a consultation is the only way to know properly.
We do not approach shoulder arthroscopy surgery as a default response to shoulder pain. If there is a realistic chance that further physiotherapy, a different injection protocol, or activity modification will get the shoulder to a functional place, we explore those options first and support you through them properly. Surgery always comes with recovery demands, and it should not be undertaken unless the benefit clearly justifies that.
Where we do recommend moving forward is when the situation fits a pattern we recognise. Conservative treatment has been done properly and has not achieved enough. Imaging confirms structural damage that is not going to resolve without intervention. The shoulder is consistently disrupting sleep, limiting work, or cutting across things that matter to the patient’s daily life. Or the problem is simply the kind, a full thickness tendon tear, a significant labral injury, a structurally unstable joint, that conservative treatment was never going to fix adequately in the first place.
If any of that sounds like your situation, the conversation is worth having.
Before and During the Procedure
We complete a thorough pre-operative assessment before anything else. Blood work, medical history, imaging review, an anaesthesia discussion personalized to your specific situation. You receive clear written instructions for the days before surgery. What to avoid eating and drinking. What to arrange for getting home. What to bring. Who to contact if something comes up. We do not leave patients to navigate this on their own.
On the day, once anaesthesia is established, the incisions are made and our surgeon examines the full interior of the joint before beginning any repair. This step matters more than people might think. MRI and other imaging are valuable, but they do not always show the complete picture. The live arthroscopic view sometimes reveals additional findings that adjust or refine the plan. Seeing the problem directly, in real time, is a different level of information.
The repair itself might involve reattaching torn tendon tissue, trimming or smoothing damaged cartilage, releasing a thickened capsule, removing inflamed tissue, clearing bone spurs, or tightening loose ligaments. Often it is a combination. The shoulder surgery with arthroscope typically runs between one and two hours, though complexity varies and we do not rush.
Recovery, Without the Vague Reassurances
We are asked about shoulder arthroscopy recovery time constantly, and we understand why. People want to know what they are actually signing up for.
The straightforward answer is that recovery depends heavily on what was repaired. A decompression for impingement and a full rotator cuff reattachment are genuinely different procedures in terms of what healing demands from you. What we can offer is an honest general picture.
The first two weeks are about protecting the repair. The arm stays in a sling. The shoulder is swollen and tender and that is expected. Ice helps considerably. The medication plan we send you home with manages the discomfort well for most patients. This is not the phase to test boundaries, and patients who try to rush it almost always regret it.
From weeks two to six, physiotherapy starts. Sessions begin gently, working on maintaining movement without stressing the repair, then progress according to how each patient is actually recovering rather than a fixed schedule. Our rehabilitation team is involved throughout this phase and adjusts the programme as you go.
Between six weeks and three months, strengthening work builds progressively. Most patients managing desk-based work or light daily tasks feel relatively normal during this period. The shoulder starts feeling like it belongs to them again.
Athletes and those doing physical work typically reach full function somewhere between three and six months. We use objective assessments of strength and range of motion to determine return to sport readiness. The calendar is a rough orientation, not the deciding factor.
The most consistent thing we observe in our patient outcomes is this: the patients who engage properly with physiotherapy, who show up and do the work, recover noticeably faster and reach a higher level of shoulder function than those who treat it as optional. Not marginally. Noticeably. Every time.
Benefits Worth Naming Plainly
The shoulder arthroscopy benefits are well documented and, in our experience, match what the clinical evidence says.
Smaller incisions leave the surrounding healthy tissue largely intact. The body has a fraction of the damage to repair compared to open surgery, and that directly translates to less pain, less swelling, and a more manageable recovery from day one.
Going home the same day matters more than it might sound. Recovering in your own environment, in your own bed, with familiar surroundings and people around you, is meaningfully better for most patients than days in a hospital ward.
Less postoperative pain means less reliance on strong medication. Clearer head, better sleep, more active participation in your own recovery from earlier on.
And the combination of diagnosis and treatment in a single session is genuinely efficient. One anaesthetic, one recovery, one rehabilitation process. Not a diagnostic procedure followed by a separate surgical one weeks later.
The Risks, Stated Directly
Shoulder arthroscopy risks in experienced hands are low. They are not absent, and we think pretending otherwise does patients a disservice.
Wound infection is uncommon and almost always treatable with a course of antibiotics when caught early. Temporary nerve irritation causing tingling or numbness in the arm is possible and typically settles on its own over weeks. Stiffness can develop if rehabilitation is delayed or done inconsistently, which is one of several reasons we take the physiotherapy side of recovery so seriously. In patients who smoke or have conditions like diabetes that affect tissue healing, the risk of incomplete repair healing is higher, and we discuss that directly if it applies. Anaesthesia carries a small degree of risk for everyone, screened for and managed carefully by our team.
We go through this honestly at the consultation. Bring your questions.

Before

After
Why Trusta Clinic
No list of credentials here. Just the honest version.
Our shoulder specialists focus on joint conditions and arthroscopic surgery. Not occasionally. It is the concentrated focus of their practice, and that specificity shows in consistent outcomes.
We keep your care coordinated under one roof from the first appointment through the last physiotherapy session. The surgeon who operates on your shoulder is directly connected to the team rehabilitating it. Things do not fall through gaps.
We tell you what we actually think. That includes telling you when surgery is not the right answer yet. We would rather lose a procedure than recommend one that is not genuinely in your interest.
And the relationship does not end when you leave the operating room. Recovery matters as much as the surgery itself, and we remain actively involved throughout it.
A Few Common Questions
How painful is the recovery, really?
Milder than most patients expect. The first week involves real aching and stiffness, managed well with the plan we send you home with. Most patients tell us afterward it was easier than they had prepared for. Sharp or worsening pain is not expected and we want to hear about it if it happens.
When can I drive?
Generally somewhere around four to six weeks, once the sling is no longer needed and the arm has enough reliable control. This varies based on which shoulder was operated on and what was repaired.
Is physiotherapy compulsory?
It is as compulsory as anything in medicine gets. The surgery repairs the structure. Physiotherapy teaches it to function under real load again. There is no shortcut around this part, and we have seen enough outcomes on both sides to say that clearly.
Will the repair hold long term?
Yes, for patients who complete rehabilitation and take reasonable care of the shoulder going forward. We do not do temporary patches. The repairs are intended to be durable, and for the vast majority of patients they are.
What if I am anxious about having surgery?
Many patients are. Write your questions down before you come in. Bring them all. We would rather spend an extra thirty minutes making sure you feel genuinely informed and settled than have you go into the procedure carrying unresolved worry about something we could have addressed in the consultation.
Book a Consultation
If you have been managing your shoulder rather than fixing it, and you are ready to find out whether there is a better option, come and talk to us.
Book your consultation with Trusta Clinic in Dubai. Bring your scans if you have them, bring your questions, and tell us honestly what the shoulder has been doing and how it has been affecting your life. We will examine it properly and give you a straight answer about what is going on and what we think you should do about it.
That is all a first appointment needs to be.
